


Mapping of Lymph Node Metastasis From Esophagogastric Junction Tumors: A Prospective Nationwide Multicenter Study
Title: Mapping of Lymph Node Metastasis From Esophagogastric Junction Tumors: A Prospective Nationwide Multicenter Study
Authors: Yukinori Kurokawa, Hiroya Takeuchi, Yuichiro Doki, Shinji Mine, Masanori Terashima, Takushi Yasuda, Kazuhiro Yoshida, Hiroyuki Daiko, Shinichi Sakuramoto, Takaki Yoshikawa, Chikara Kunisaki, Yasuyuki Seto, Shigeyuki Tamura, Toshio Shimokawa, Takeshi Sano , Yuko Kitagawa
Journal: Annals of Surgery, Vol 274, Issue 1 (2021)
DOI: 10.1097/SLA.0000000000003499
Abstract:
Objective: The aim of the study was to determine the optimal extent of lymph node dissection for the 2 histological types of esophagogastric junction (EGJ) tumors based on the incidence of metastasis in a prospective nationwide multicenter study.
Background: Because most previous studies were retrospective, the optimal surgical procedure for EGJ tumors has not been standardized.
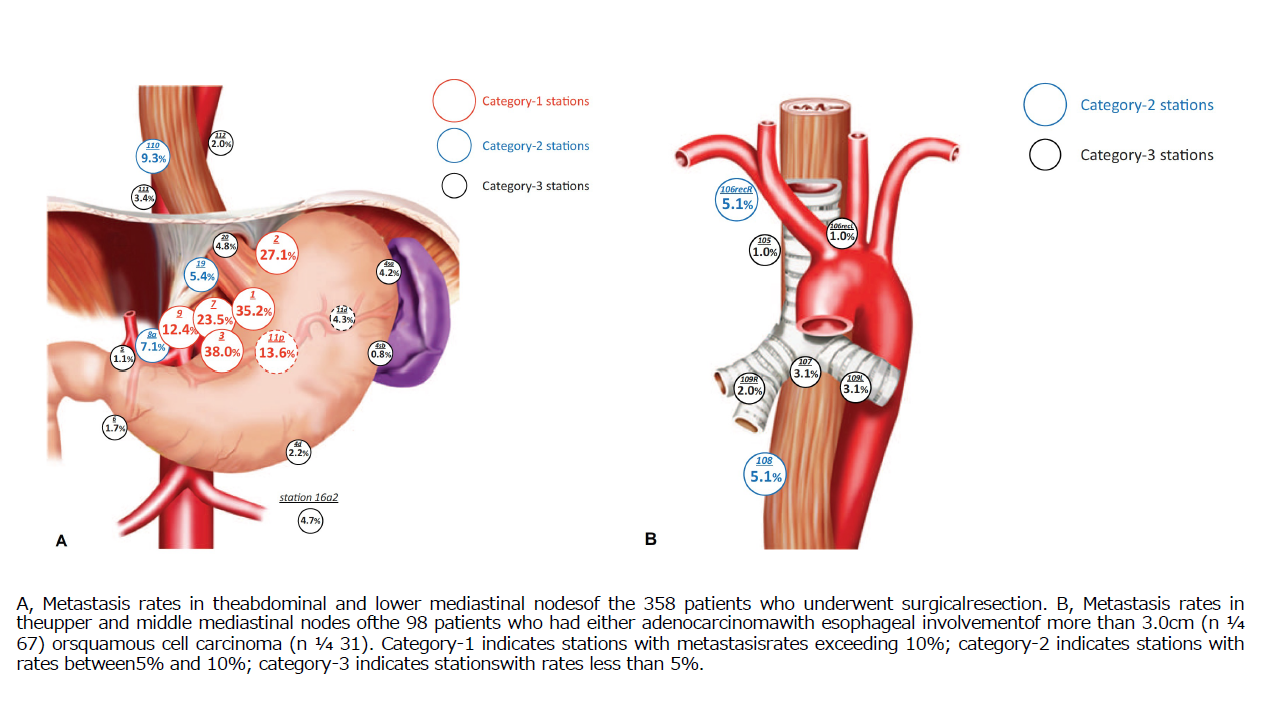
Methods: Patients with cT2-T4 adenocarcinoma or squamous cell carcinoma located within 2.0 cm of the EGJ were enrolled before surgery. Surgeons dissected all lymph nodes prespecified in the protocol, using either the abdominal transhiatal or right transthoracic approach. The primary endpoint was the metastasis rate of each lymph node. Lymph nodes were classified according to metastasis rate, as follows: category-1 (strongly recommended for dissection), rate more than 10%; category-2 (weakly recommended for dissection), rate from 5% to 10%; and category-3 (not recommended for dissection), rate less than 5%.
Results: Between 2014 and 2017, 1065 patients with EGJ tumor were screened, and 371 were enrolled. Among 358 patients who underwent surgical resection, category-1 nodes included abdominal stations 1, 2, 3, 7, 9, and 11p, whereas category-2 nodes included abdominal stations 8a, 19, and lower mediastinal station 110. If esophageal involvement exceeded 2.0 cm, station 110 was assigned to category-1. Among 98 patients who had either adenocarcinoma with esophageal involvement over 3.0 cm or squamous cell carcinoma, there were no category-1 nodes in the upper/middle mediastinal field, whereas category-2 nodes included upper mediastinal station 106recR and middle mediastinal station 108. When esophageal involvement exceeded 4.0 cm, station 106recR was assigned to category-1.
Conclusion: The study accurately identified the distribution of lymph node metastases from EGJ tumors and the optimal extent of subsequent lymph node dissection.
Related Articles:
- Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal andabdominal transhiatal approaches to total gastrectomy for adenocarcinoma of theoesophagogastric juncti on or gastric cardia. British Journal of Surgery, Vol. 102, Issue. 4, pp. 341-348 (2021). DOI: 10.1002/bjs.9764
- Results of a nati on-wide retrospecti ve study of lymphadenectomy for esophagogastric juncti oncarcinoma. Gastric Cancer, Vol. 20 (Suppl 1), pp. 69-83 (2017). DOI: 10.1007/s10120-016-0663-8
- Theoretical therapeutic impact of lymph node dissection on adenocarcinoma and squamous cell carcinoma of the esophagogastric junction. Gastric Cancer, Vol. 19, pp. 143-149 (2016). DOI: 10.1016/j.expneurol.2021.113834